I would rather make a difference than be acknowledged as being right
In the daily update I included my up to date “optimism scale”. This is a scale that can move daily depending on latest developments. Extreme pessimism of 1 would entail confirmation that the virulence of the virus is such that infections result in a mortality rate of 1% or greater (10x the virulence of severe flu) even under optimal conditions, continued indications of very high transmissibility (a reasonable proportion of infected individuals infect several people), and a lack of effective treatment and/or prevention (vaccination). An increase in optimism would necessitate clear evidence that outbreaks outside of China were being contained, evidence supportive of a virulence attenuation resulting in a mortality rate of below 1%, or strong indications of successful therapeutic treatments that can be administered widely and rapidly.
My optimism/pessimism level – from 10 to 1 in decreasing optimism – was increased today to 2.
This is my equal highest level of optimism since I commenced writing updates on 9 February and I have raised the level to 2 because there have been (mixed but overall) positive developments around vaccines and already nationwide vaccine programs have commenced in the UK and USA. The reader should, however, consider the nuance around these developments below.
18 December (My Final Report)
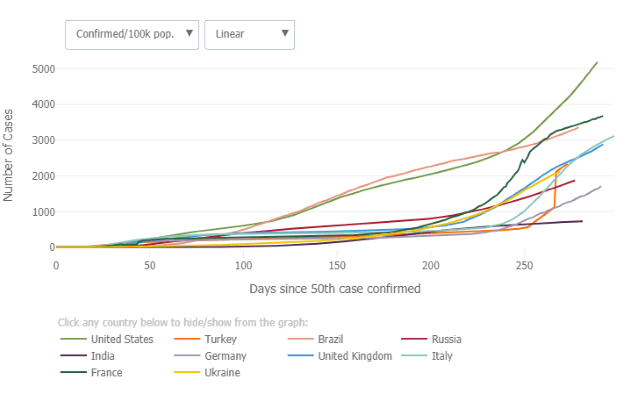
WHO dashboard shows that as at 5:05 pm CET 17 December, there have been 72,851,747 confirmed cases globally with 1,643,339 deaths.

It is with much sadness that I discuss the current situation. It is a bleak Winter in the Northern Hemisphere, to say the least, and the festive season is undoubtedly the most sombre in decades, probably since the depths of WWII. Sadly politics has impeded the pandemic response in many nations – usually based on a divide between conservatives placing higher importance on the economy (or at least perceptions of measures impacting on the economy) and parties left of that position placing a higher value on human life. When those differences are expressed across the layers of Government – e.g. Federal v regional – paralysis has been common. For example, the lack of leadership at the Federal level severely impeded the US response, and threatened to do likewise in Australia (but the vestiges of State autonomy ensured the Premiers could not be strong-armed by PM Morrison, thankfully), whereas Angela Merkel’s efforts in Germany to protect people from the ravages of the pandemic have been hampered by obstructionist regional politicians.
In my earliest reports I discussed potential seasonality to the pandemic as I was acutely aware that the Southern Hemisphere would be the first to face a full Winter with the global pandemic. Seasonality has very clearly been a major factor in the major temperate population centres in the Northern Hemisphere. The Summer lull in the pandemic, especially in Europe, was brought to a shuddering end as case numbers exploded in mid-Autumn catching virtually all nations off-guard. While the sharing of information on best practice for treating COVID-19 developed through the year has resulted in slightly better outcomes for severely ill patients, these gains are threatened by the sheer numbers of hospitalised patients such that hospital systems in most European nations and North American regions are on the brink of being totally overwhelmed. Exhaustion amongst the real heroes of this crisis – the health care workers – is a major concern everywhere.
National political leaders are attempting to balance the need to impose tougher and tougher restrictions to lessen the pressure on their health systems with pandemic fatigue, despondency or out and out anarchy amongst certain groups of citizens (in some cases which they, themselves, played a part in stoking – hey Borris?) While the overnight news that yet another national leader, French President Macron, has been infected is a reminder that nobody is immune, the knowledge that such elites within society will receive an entirely different standard of care to the majority only proves the necessity for change through this period, which I began to call in March “The Great Reset“.
Those who celebrate Christmas this December will be hoping that, while experiencing a grim festive season, they might find in their gift stocking not coal but a solar panel and the hope of a brighter future…
As foreshadowed in previous Coronavirus updates, this will be my final one.
Firstly I will point out that this is now the only update on this landing page. All previous updates are on the linked pages (in reverse chronology starting here) because I updated the material at the head of the page which had stayed constant since much earlier in the pandemic.
In those first few weeks of the pandemic I initiated an “Optimism Scale,” which in my first update was at the penultimate level of pessimism until 24 February when I downgraded it to 1 indicating extreme pessimism, when the WHO Situation Report No. 34 listed 17 COVID-19 deaths outside of China. In doing so I stated
this could be upgraded with some unexpected development, but the information emerging out of especially Korea, Italy and the middle-east is very concerning which confirms rapid and widespread transmission, including in well developed countries, with the clear suggestion of high mortality rate
Having left my optimism level at 1 for almost 10 months, I have now raised that rating to 2.
That is in no way indicative of the current situation with the pandemic raging globally, especially in the Northern Hemisphere, including in the developed nations within North America and Europe.
It is an indication of my optimism that, on a global basis, things may be set to improve once the Northern Hemisphere passes the critical Winter/early Spring period.
While my own optimism is genuine, I do need to note that it is not nearly as strong as sections of the Australian media and broader society have allowed themselves to indulge in. While a certain level of optimism is both “earned” and understandable, at times it has bordered on euphoric which is ill-advised.
What follows is my honest optimistic view for the way forward, but it is heavily qualified by significant nuance in both volume and salience.
In my 30 June Coronavirus Update I said that I knew the pandemic was a multi-year event from the outset, but leaving the year from the heading of my updates was intentional as “I simply had no intention of writing updates beyond the first year of the pandemic because I knew it would be too depressing”.
In my previous Coronavirus Update I said that for my final update I would recap all of my Coronavirus updates and other writing on the pandemic before going on to give my views on the year(s) ahead.
I have decided to drop the first part because I think to do so is inappropriate. Such a conspicuous lack of humility, in this difficult time for humanity, is not really authentic to my true self. In my writing, where I have quoted myself from earlier papers, it has mainly been to show that I have been prescient in relation to the COVID-19 pandemic to implore the reader to take on board my views.
Most importantly I prefer to devote my energies to looking forward to the future.
Before I do that, however, I do need to briefly mention an upcoming post. As a complete outsider it is difficult if not impossible to gauge the impact of my works and words. I noted in “Evidence of MacroEdgo Impacts” that an Australian researcher based in Singapore led a team which showed that the concerns that I raised earlier about the potential for meat processed in facilities where there are large numbers of infected workers is a risk for seeding clusters was justified.
Now I note that in June the World Economic Forum (WEF) launched an initiative they have titled “The Great Reset”. This initiative is essentially identical to the approach that I called for in my essay of the same title which I posted on 30 March.
I will discuss these developments in a post which I will release next week. But at this early stage let me just say that no, I have never had any contact with the WEF, or anybody else about the initiative or any other similar initiative; and yes, I am pleased to see that many global actors have increased their activities to argue openly about what shape we want to emerge from this major global humanitarian event.
Given the friable environment in which these discussions are occurring I feel I need to pre-empt some of what I will say in that upcoming post. To the conspiracy theorists on either and all sides, I need to tell you that you are barking up the wrong tree in believing others who tell you that all of this is part of an orchestrated strategy.
Rare and unpredictable shocks to individuals usually cause them to reflect on their lives, and when that shock occurs to societies collectively people will naturally question whether our societies are heading in the right direction.
That is nothing to be feared. It is to be embraced as a human being because much good can come from it when there is authentic open engagement.
I will discuss this in much greater detail in my post, but it should be clear to all that joining a social media group that adopts extreme positions that are simple and clear-cut on these very complex issues, and where participants do not engage in open respectful dialogue with any and all others that show them respect and who raise valid points, is not a way to become genuinely informed and participation on that basis is unwise.
The criteria for my optimism scale are mortality rate (i.e. infection fatality rate – IFR) and progress at developing cures (including vaccines).
The reason for upgrading my optimism level is based almost exclusively on vaccine developments.
The virulence (or lethality) of the novel coronavirus has been one of the most contentious issues from the earliest days of the pandemic, worsed by a disappointingly large number of political leaders downplaying this aspect.
I chose a rather arbitrary (and round number) of 1% as the bar to fall below to raise my optimism level. Early estimates of the IFR varied significantly, but with a year passed I doubt that estimates will be any more accurate (though I expect that debate over these estimates will never be settled).
Of course, also, the IFR experienced in different regions will be impacted by an enormous range of factors from natural (e.g. weather/environmental) and socioeconomic (including dispersion/homogeneity of those factors – i.e. societal inequality). Moreover, treatments (including “incomplete cures” or “cures under development”) and their interaction with these other factors will also affect the IFR over time. All of this has been discussed in early “Coronavirus updates” and my other reports.
I will point out, however, that even in developed countries in the Northern Hemisphere many countries are approaching full capacity in their intensive care wards from COVID-19 patients. I was shocked to learn that Sweden, a country known for having one of the highest standards of health care in the world, has recently sent patients to other Nordic countries. Of course, Sweden is well known for their adoption of very light social restrictions through the pandemic which they have persevered with until only recently. The point is that even in countries with excellent health systems the IFR can increase when their well provisioned and staffed hospitals are overwhelmed. And on that point, sadly Sweden now faces a crisis amongst their health workers who are resigning due to exhaustion.
I have consistently placed a high value on the research out of the Imperial College London, and this is from their latest report on the subject:
we estimate the overall IFR in a typical low-income country, with a population structure skewed towards younger individuals, to be 0.23% (0.14-0.42 95% prediction interval range). In contrast, in a typical high income country, with a greater concentration of elderly individuals, we estimate the overall IFR to be 1.15% (0.78-1.79 95% prediction interval range).
I would not become less pessimistic based on these figures. Moreover, history would suggest that, and it will undoubtedly be repeated unless the world changes a great deal and rapidly, the IFR in low-income countries is unlikely to fall appreciably in the near future (though I am getting ahead of myself).
Now to the vaccines and I must start with an admission. A week earlier when I began thinking of drafting this final update I was toying with increasing my optimism level by 2 places to a level of 3. That was due to just how surprisingly positive was the run of data releases on the vaccines under development. There has been a run of setbacks since, which has brought us all back to Earth a little, and it was a lesson to me also on the need to keep optimistic emotions in check.
I will detail all of this below, but let me just say very clearly that even two months ago if you dumped all of these data on me to consider at the same time, I would have come away feeling cautiously optimistic and thinking that the vaccines show greater potential than I had dared to hope previously.
Perhaps it is unavoidable, but receiving updates in drips and drabs leaves us all prone to feeling like we are riding roller coasters. That is why I believe it is incumbent on political leaders and health officials to be calming voices of realism when positive developments occur, and to store the optimism mainly for use when we receive setbacks.
Unfortunately many modern politicians seem only capable of cheerleading and pulling blinkers over eyes in a vain attempt to create (consumer) confidence, whether it be justified or ill-advised. Here I do have to note that this refers mainly to male leaders and it reminds me of my desire to expand on the gender differences in leadership through the pandemic as an extension to my article “Toxic Masculinity and Political Footballs“.
The new class of vaccines based on mRNA (messenger RNA, a type of nucleic acid present in all cells of all living organisms in the world, like DNA) shows enormous promise with both the BioNTech/Pfizer vaccine and the Moderna vaccine achieving an efficacy of over 90% at preventing COVID-19 disease (but not necessarily preventing infection) across age groups and ethnicities.
There are flies in the ointment, however: will vaccinated people still become infected and transmit infection to others (including potentially unvaccinated people); how long will protection from developing COVID-19 last; because this is new technology significant quantities of this type of vaccine have never been produced so what will be the production rate over the next year or two; given protection might wane, will production ever be able to meet the demand for people who want/need to be vaccinated (including with booster shots); being a new class of vaccine and requiring quite specific handling which requires significant logistics, just what proportion of humanity could realistically receive this type of vaccination; on the first day of rollout in the UK two people who had severe allergies had adverse reactions – how common might this be, and what other complicating factors will emerge as the vaccine is rolled out to millions of people.
Note that I have little concern over safety for these vaccines, but we should always expect that we are going to learn of complicating factors, which hopefully will be relatively minor and/or rare, when hundreds of millions of people receive new treatments.
It is difficult to escape the view, however, that while this class of vaccine will likely become the gold standard for preventing COVID-19, it may only be given to the highest risk (of developing severe disease or of exposure to the virus) members of society in high-income developed countries. Even that is dependent on further developments being broadly positive which is not guaranteed.
I found this to be a brilliantly clear explainer on early COVID-19 vaccine efficacy data and especially how the final efficacy could be markedly different depending on how long the immune response lasts.
But again, this is a great start and we would have much less reason for optimism without it!
It follows that the majority of humanity will likely be highly reliant on success with the other vaccines. And there are very many of them – almost 200 in fact – being developed both in Western developed countries as well as in India, China and Russia. I will just concentrate on what is known from the final stage trials that have been released as well as the pertinent to Australia UQ/CSL vaccine.
The most promising – to this point – of the remaining vaccines is one by Oxford/AstraZenica. Unfortunately its data release was not well handled, which given the febrile environment, has led to a degree of scepticism in even informed sections of the general and scientific community. The issue is that around 20% of participants who received the vaccine received a half-strength initial dose – which now appears to have occurred because of an error in manufacturing – and those who received the lower initial dose displayed a higher level of efficacy. However, there are further issues in that most of these were younger. In short, these missteps, that were always going to become public knowledge due to the extreme level of interest in vaccine development, have made it clear that we really are in an accelerated development mode and that mistakes and vagaries, especially when dealing with a pathogen known to mankind for just one year, are highly likely to occur.
Nonetheless, it should not be lost that the statistical significance and the overall efficacy rate of around 70% is quite acceptable. In fact, this was about the best result that I dared hope for before the data on the mRNA vaccines was released. Moreover, this is a cheap vaccine which requires no unusual storage or supply conditions so this may be a vaccine “for the masses” including in the developing world.
Researchers have started another full trial to determine the efficacy when all participants who receive the vaccine received a half dose initially, so that might suggest that the work is incomplete. But in reality all of the vaccines will continue to be the subject of further research to continue to determine the finer details, such as how effective they are at reducing infections and transmission.
The Russian and Chinese vaccines have been rolled out in their respective countries. To be used in most western countries I imagine that they will be required to undergo trials in those countries. Whether that occurs will largely be determined by success with the other vaccines. These will likely have a higher uptake in low-income developing countries as and when confidence grows in them from use.
Finally we have some more disappointing results. The GlaxoSmithKlein/Sanofi vaccine suffered a serious setback last week as it failed to produce significant protection in the vulnerable 60+ year cohorts, and this has knocked their timeline to release back by at least 6 months.
Disappointing for Australia especially, the UQ/CSL vaccine has been abandoned because its use resulted in false positives for HIV. I understand that researchers will persevere with the technology, but the setback was so serious that it is unrealistic that it will play a part in the management of the COVID-19 pandemic.
To finish this section on a positive note, it is great to see that within a year of the onset of this pandemic residents of the UK and USA are already receiving injections as a part of a national vaccination program. That is an enormous feat for humanity!
All of this was made possible by the excellent work of the scientists at the Wuhan Institute of Virology, led by Dr Shi Zhengli, who first identified the virus and made the entire genetic sequence available to the world within weeks. To those who have not read that original article in Nature, I suggest you do so even if you have no virology or even a science background – the enormity of the studies that these scientists performed in the space of just a few weeks is readily apparent and is nothing short of remarkable.
To conclude I will expand on my views on how the pandemic is likely to progress next year and after.
In “How Society Will Change If A COVID-19 Vaccine Is Elusive” I dared to wonder about an Australia where we have a new normal that is closer to the life that we have lived in 2020 than the one we had before it. Until the preliminary final stage vaccine trial results for the mRNA vaccines were released, I feared that such a reality was an uncomfortably high probability. And when I undertook to put together these thoughts I believed they would be more sobering.
Right now it appears that the more concerning scenario is less likely because scientists, standing on the shoulders of those around and before them, have performed an incredible feat in developing excellent and safe vaccines in under a year from the commencement of the pandemic.
That is not the end of the story, unfortunately, as above I discussed some of the many questions that remain unanswered about how the vaccine works and interacts with the human immune system. While these are significant questions, which will not be fully answered by the end of next year, even more critical questions relate to the virus itself.
From my earliest updates and reports I have discussed the reality that the virus will mutate as it spreads and these mutations could have implications for how quickly it spreads or how ill people become. Those mutated strains could be advantageous for our management, or they could complicate it and thus worsen the pandemic.
Scientists are finding that for an RNA virus this coronavirus is not mutating as much as it might have, which is good news. It is now so widespread, however, that the potential for mutation is very significant. That is further complicated by an additional factor.
In “COVID-19 Risks With Animals” I discussed that the virus has a very broad potential host range, meaning that the virus has infected many different animal species and predictions are that it could potentially infect very many more animal species if conditions for exposure existed. The more the virus spreads in humans, the greater the chance of exposure to a broader range of animals. And the more other animals are exposed, the greater the chance of them acting as reservoirs for further infections in humans, and the greater the chance of more significant mutations occurring so that more different strains re-emerge in humans.
While the news media is reporting vaccine successes, we are also learning about new strains of the virus that have been detected which may be different enough from the initial strains that they have implications either for how many people may become seriously ill and die, or, perhaps even more important now, how effective will be the vaccines against these strains because the vaccines were made using much earlier strains of the virus.
This quote from a UK scientist explains the urgency around a recently detected strain:
We think there’s a mechanism for the virus to start escaping,” said Ravi Gupta, professor of clinical microbiology at the Cambridge Institute of Therapeutic Immunology and Infectious Disease at the University of Cambridge. “We need to crack down on it. We don’t know what it’s going to do long term but we can’t take a chance on it. It’s unlikely it’ll make people sicker, but it could make it harder to control.
These mutations are being monitored by the scientific community. Of course the vaccines can be reworked to be more effective against emergent strains, but that will still take time even in a streamlined process. In an all too plausible scenario, and given the reality that we do not yet know the production rate for mRNA vaccines, we may find ourselves continually behind if the vaccines must be continually reworked (as is required for flu vaccines).
This novel coronavirus is now highly unlikely to ever be eradicated because that would require a very cheap and easily delivered vaccine effective against the full range of strains, which prevents infection, being delivered to almost all humans and potentially exposed animal populations.
That is highly improbable.
I do wonder what will be the way forward in low-income developing countries, where the effects of the pandemic are already under-reported in the media compared with wealthy developed countries, especially once the shock to humanity begins to subside.
History has shown that wealthy countries tend to quickly lose interest in assisting developing nations, because when citizens’ focus moves their elected officials feel no incentive to assist, and the hard work of engaging wealthy countries in vaccination and other health programs is left to activists and their organisations.
There is one factor, however, that currently exists which has not been the situation for decades; that is the battle for hearts and minds, and ultimate geopolitical influence, between Western nations and China that I discussed in “Investment Theme: Developing Asia ex-China“. (Briefly re-reading this post reminds me of how necessary it is that I quickly complete the post that I am drafting restating my views on China in light of the pandemic and Trump’s exit.)
For humanity in aggregate, and especially the wealthy developed nations with older age-structured societies making them more vulnerable to COVID-19, the best management strategy for COVID-19 is to minimise its spread everywhere on Earth, thereby cutting down its opportunity to mutate sufficiently to perpetuate or reignite a pandemic. However, if the pandemic were even briefly arrested in the developed world it would be consistent with history for the developing world to be left to their own devices to battle COVID-19 impacts. I am more optimistic than I normally would be that high-income countries will remain engaged with battling COVID-19 in low-income developing countries. But there are even bigger question marks on how successful those efforts might be.
As detailed above the vaccines that have shown the highest efficacy at preventing COVID-19 thus far are expensive and require logistics and facilities that will preclude their use outside of developed countries. How beneficial to the developing world will vaccination be is dependent on the effectiveness of vaccines that can be easily rolled out in challenging circumstances. And the significantly lower mortality rate (IFR) from COVID-19 observed in low-income developing nations may mean that, unless the efficacy is very high, the benefits of a vaccination program to the individual and the low-income nation may be limited.
Ultimately how widely COVID-19 vaccines are administered in the developing world will depend on the balance of costs and benefits of the vaccine program, and the willingness of the developed nations and other geopolitically active nations to derive goodwill from such programs.
We head towards the closing of 2020 in a truly terrible situation, and I constantly find it disheartening that still there are human beings who suggest that their own desires and beliefs outweigh the pain of so many other human beings.
Through this year my subconscious has struggled to come up with a single, simple statement on this and I only a achieved that in recent weeks:
Those who argue for minimal or no measures against COVID-19 are in reality saying “the extra risk to everybody’s health is worth it to me”.
Obviously there has been much said this year about the collective good versus individual rights, and this debate will surely go on in earnest for many more years. My views are clear in my writing and need no further explanation here.
I will simply make two points. Firstly that the innocuous yet invaluable hygiene device of a face mask has become the symbol of individuals’ rights will in retrospect be seen for what it is – plain stupid – and not unlike burning books!
Secondly, the plain numbers of confirmed cases and deaths on various dashboards, while shocking in their enormity, can in no way ever begin to reflect the true loss to humanity. That loss extends well beyond the people who these numbers represent to the years of life cut shorter than otherwise, and to what they might have done and achieved in that time.
The British anthropologist Robin Dunbar is known for developing a guide for the typical number of relationships that humans maintain through their lives. He found that on average each human being maintains relationships with an average of around 150 people at any one time. Of course there are different depths of relationships that we maintain, with our nearest and dearest amounting to 3 to 5 people, and then a further very close 15 friends with whom we maintain ongoing close relationships. Nonetheless connection with all the approximately 150 people in our circle provides us with the feeling of connectedness with the community.
Of course as in all things research, others have come up with different numbers, some less, many larger.
The point that I am making, however, is that if one multiplies the number of people who have died from COVID-19, the official figures for which are likely understated, by their number of contacts then we will begin to develop a truer picture of our human loss. Of course the extent is greater again because the contacts of all who have faced serious challenges against the disease have been anguished. And I think all people of good character have felt a great deal of anguish and pain for their fellow human beings who have experienced direct loss.
I know that some will talk about the anguish and pain associated with apparently lost or diminished ambitions as a consequence of measures in response to the pandemic. To that I would say that perspective needs to be given to the fact that those ambitions are not necessarily lost or diminished but delayed.
The ambitions of those people who pass in the pandemic most certainly are lost. And the pain of loss for those left behind will persist for their entire lives.
I have attempted to be clear and thorough about the issues that will determine how humanity progresses with this pandemic in the years ahead. Vaccines have always presented our brightest of hopes, and while progress there has been truly remarkable, we need to remain duly mindful that, without an unlikely level of luck, vaccines will not take our lives back to the way they were in 2019.
Besides the fact that we are forever changed for this experience – and that is something that I implored my readers in February to accept as soon as possible, that “the world has changed” – our road back to living a life without a thought of the novel coronavirus creeping into our minds on a daily basis, like when we greet somebody whether they be friend or acquaintance, or when we shop, remains several years away.
However, and it is a big however, I do believe that once this northern hemisphere Winter has passed then we probably have passed the worst of the pandemic impacts on us, if for no other reason than our expectations have been reset.
My predictions on how and when we might be able, or perhaps might feel safe, to do things such as travel internationally are pointless because the answers to those are in part related to politics and otherwise are dependent on our own views on risks and rewards.
What is clear is that increasing proportions of citizens – not necessarily inhabitants or residents – of high-income developed countries will have the opportunity to be vaccinated with vaccines that are highly effective at preventing disease at least in the short-term. What proportions of citizens in each country are (or remain) protected from either disease or infection at the end of 2021 is impossible to know.
The one thing that I do know for certain is that next year, and likely for several more years, high-income nations where residents want to minimise human loss will need to guard against complacency and be prepared to continue to be adaptive and innovative in responding to the pandemic, along the lines that I outlined in my campaigns “Make This Summer Count!” and “We Mask Because We Care“.
While I realise that a reader disinclined to agree (in general) with my views is unlikely to have read through to this point, if they have I would point them to an article co-authored by Prof. Ian Frazer AC which makes some of the points that I have made above and strongly recommends the very same approach that I have been advocating since launching these aforementioned campaigns.
Thank you to the scientists who have given their all this year. Thank you, also, to the authentic leaders in this world who may be elected decision-makers, appointed Government officials, members of the business community, and members of the broader community. (Yes, implied in my statement is a view that those who do not believe in the primacy of human life do not meet my definition of authentic.) And finally, thank you to my fellow residents of Australia, and of many other nations, who in their great majority did authentically show that they cherished human life and connectedness.
Previous Coronavirus (COVID-19) Updates
Coronavirus (COVID) updates from:
Gained value from these words and ideas? Consider supporting my work at GoFundMe
© Copyright Brett Edgerton 2020

You must be logged in to post a comment.